More Specialist Toolkits
Mutational Toolkit | Questions Toolkit
Dear fellow patient,
A cholangiocarcinoma (CCA) diagnosis can be overwhelming, but you are not alone. Our toolkit is designed to help guide you forward with the gift of knowledge, experience, and wisdom from fellow patients and caregivers who have been in your shoes.
Bridging the Cancer Information Abyss
The CCA Toolkit app provides a roadmap and a bridge to a pathway traveled by other cholangiocarcinoma patients. Our goal is to better equip and empower your capacity to mount an effective and robust response to your diagnosis.
Ultimately you are the captain of your own ship, and you need to lead this challenge – others will follow your lead. Be open-minded, be willing, be consistent, and trust yourself.
Steve Holmes
Fellow Patient

A Gold Standard Knowledge Pathway to better decision making
Being an informed patient means you understand the information in a way that you can proactively act on it to make better quality decisions. This is the first crucial step towards becoming an “Empowered Patient.”
Think of the content below, as sequential stepping stones of knowledge. Understanding this sequence will greatly improve your understanding and provide a significant advantage in your interactions with medical professionals and subsequent decision-making.
- DNA: We are all individually uniquely DNA coded. This makes us who we are.
- DNA Replication: Our DNA is constantly making copies of itself.
- Replication mistakes in copying DNA often happen due to things like sun exposure, smoking, what you eat, and even stress.
- DNA Spell Checker: Think of your immune system as a DNA spell-checker, fixing errors and getting rid of cells that can’t be fixed.
- Unrepaired Mistakes: When the Immune system misses or is unable to repair a DNA mistake, the cell becomes mutated (bad rogue cells) and will continue to grow and multiply unchecked.
- Mutations: These rogue cells can become tumors, and some may turn into cancer.
- New technology can spot these DNA errors through special tests like immunohistochemical (IHC) analysis and molecular profiling.
- IHC (Immunohistochemistry) is a quick lab test using special dyes to find abnormal proteins (Biomarkers) in tissue samples.
- Molecular profiling dives deeper into the tissue sample, looking at the tumour’s genetic makeup to find what might be causing the cancer.
- Tissue samples These samples are usually taken during surgery or a biopsy. If that’s not possible, blood tests are another option. increasingly, it can also provide ctDNA information (ct = circulating tumour) which is tumour shedding material in the blood.
- ctDNA: “Blood tests look for ctDNA, which is basically pieces of the tumor floating in your blood.”
- Pharmaceutical: Drug companies are always working on treatments that target these specific mutations.
- Immune support: This treatment boosts and supports your immune system to help it spot, target, and eliminate cancer cells it has missed or has managed to evade detection.
A Pathway to Inner Strength and Resilience
Attitude is an essential ally in combating cancer. The following insights are distilled from observations of patient success, serving as an inspirational guide.
Understanding this sequence can empower you to better navigate the unique challenges of cancer:
- Our Values stimulate our innermost willingness and visions
- Willingness drives our visions
- Vision shines a light on our direction
- Direction stimulates our purpose
- Purpose generates our inner momentum
- Inner Momentum is our first unseen momentum, it unlocks and opens us up to new thoughts
- Thoughts are things that are sensory data input from our environment, that stimulate our thinking and actions
- Thinking is the action that activates or acts on our thoughts, shaping and refining our momentum and attitude
- Attitude is the sum of our thoughts and actions, shaped by our values.
Remember, if our values form the foundations of our attitudes, conflicts in our values will/can impact our overall attitude. Keeping an attitude aligned with our values helps empower our capacity to rise above the many challenges. This alignment can make distinct differences as we move through and beyond the diagnosis.
Understanding and choosing the right caregiver is an important decision that can make a significant difference in your cancer journey. The contents of this section should be discussed and understood by you both.
What you need to know
Your caregiver should be a person who knows you well and is able to get alongside you, a person who can willingly provide assistance and support to cover your limitations both physically and emotionally.
Why do you need to know
Your caregiver will help you with your daily activities and ensure that you remain on track for your objectives.
Together you will both evolve into a team, this does take and requires pause, poise and consistency by you both.
Please remember that your caregiver will also need good support to be the best they can be.
Important note
Choosing the right caregiver isn’t just about who’s around. You both need to vibe—especially under the emotional weight of a cholangiocarcinoma diagnosis. It’s easy to just react instead of planning. Take a moment to get on the same page. Your roles will likely differ, and that’s okay. If you’re scouting for a caregiver from scratch, pick someone you can trust, someone who’s got the qualities you need.
Attributes of a Good Caregiver
Your caregiver needs to acquire specific skill sets, and often this is more about knowing what they are and fine-tuning as you go. But you also need to elevate your own game and rise above your best. When you’re at your best, it brings out the best in those around you, and this is vital in overcoming cholangiocarcinoma
When it comes to cholangiocarcinoma and surgery, it’s all about understanding your options. Surgery can be a potentially curative treatment, but it depends on where the tumour is located.
What you need to know
- Liver resection: This involves removing part of the liver where the tumor is located.
- Whipple procedure: This surgery is more extensive and involves removing a portion of the pancreas, small intestine, and bile duct in addition to the affected part of the liver.
- A combination of both: Sometimes, a combination of liver resection and Whipple procedure may be necessary depending on the tumor’s location.
- Potentially a liver transplant: In some cases, a liver transplant may be an option, especially if the cancer has not spread beyond the liver.
Why do you need to know
It’s crucial to know these options because it helps you research and understand what might work best for your specific case.
Important note
Now, here’s an important note: If surgery is a possibility but seems too risky due to the tumor’s location or size in relation to other vital organs, neoadjuvant chemo, targeted therapies, or radiation treatment may be used to shrink the tumor before attempting surgery. Seeking second and third opinions is common before making a final decision.
In summary, surgery is the primary curative option for cholangiocarcinoma, and neoadjuvant therapy followed by surgery is considered the next best option. Both have their risks, so it’s wise to seek multiple opinions to make an informed choice. The second option does carry the added risk of metastases occuring during the neoadjuvant period, which could prevent surgery. It’s a complex decision, but having all the information is key.
Attributes of a Good Surgeon
When you’re looking for a surgeon to tackle cholangiocarcinoma, there are some key attributes you should consider:
The Oncologist is the captain of your ship:
Choose an oncologist who not only knows about Cholangiocarcinoma but has current expertise and experience in treating it. Preferably, they should be actively treating patients. An experienced oncologist in cholangiocarcinoma will go the distance with you, serving not just as a short-term guide but as a committed partner who will see it through.
What you need to know
Your oncologist’s expertise and experience, communication skills, and openness to clinical trials and second opinions are all important factors in choosing the right oncologist for your specific diagnosis.
Why do you need to know
Specific expertise can mean the difference between life and death when it comes to treating serious cancer. Good communication and access to clinical trials and second opinions can also greatly impact treatment outcomes.
Important notes
- Don’t allow yourself to become just a number.
- Do not get trapped with a well-intentioned Oncologist who clearly does not have the expertise or experience – this is a common mistake and a strong reason to seek an independent second or third opinion.
- Choose an oncologist who is willing to listen to your observations, suggestions, and questions.
- When it comes to treating a serious cancer, specific expertise, experience, and attitude can mean the difference between life and death.
Attributes of a Good Oncologist
Selecting the right hospital is a critical decision for cancer patients. Often, the best hospitals are associated with top-notch surgeons, oncologists, and supporting professionals. It requires thorough research and careful consideration, tailored to your specific diagnosis. It is more than worth the effort. If you begin in a hospital due to circumstances you can still make the necessary change.
What you need to know
In making this crucial decision, consider the following key factors:
- Expertise of medical professionals in the hospital
- Available * ‘Upper GI’ resources and treatment options
- Location and accessibility
- Reputation and patient satisfaction rates
*Upper GI; Upper Gastrointestinal
Why do you need to know
Your hospital choice can profoundly influence your care. Hospitals with greater resources and expertise typically achieve better treatment outcomes and higher patient satisfaction rates. Additionally, they may provide greater access to clinical trials featuring innovative therapies.
Important note
When making your hospital selection, start by discussing your options with your GP or primary care physician. They can offer recommendations or refer you to specialists and hospitals that align with your needs.
If you find yourself in a remote area, consider hospitals that are open to collaborating with a larger hospital or oncologist in a city.
Attributes of a Good Hospital
The exact location of the primary tumour determines the subtype of Cholangiocarcinoma and the appropriate treatment pathway.
What you need to know
- Tumor Location: Understand where your first tumour began, this is known as your primary tumour
- The primary determines the exact subtype of cholangiocarcinoma and the diagnosis
- Can it be surgically removed? or has it metastasised (Spread)
- If it cannot be removed can a surgeon obtain a biopsy from it ((tissue sample)
- If it cannot be surgically removed can neoadjuvant therapy become an option
Why do you need to know
- Primary Locations determine treatment approaches
- Surgical Potential: If the primary tumor remains localised, this provides surgeons with the opportunity to remove all of the tumour
- If surgery is not an option, then ask if neoadjuvant treatment can shrink the tumor for surgery
- Seek second and third opinions before accepting that surgery is not an option – this approach also apply’s to obtaining a biopsy
- Biopsy: A Biopsy provides valuable insights into the tumour’s genetic makeup, aiding in a deeper understanding of its growth drivers and potential targeted and clinical trial treatment options. Refer to IHC testing and Molecular Profiling
Important notes
- Consult with experienced Cholangiocarcinoma surgeons and Oncologists to ensure you receive the best advice.
- Seek Second opinions only from proven experts in Cholangiocarcinoma
- Biopsy: Ask for an IHC Test and then Molecular (Genomic Profiling)
Sub-types of Cholangiocarcinoma
The location of the first tumour (Primary) determines the subtype, it is important that you understand this.
- Intrahepatic: Refers to a primary tumour that originates in the bile duct within the liver. (Learn More)
- Extrahepatic – Perihilar: Refers to a primary tumour that originates in the bile duct at the junction where the bile ducts join just outside the liver. (Learn More)
- Extrahepatic – Distal: Refers to a primary tumour that originates in the bile duct outside the liver region further down the common bile duct near the pancreas. (Learn More)
Associated Bile Duct Cancers
- Gallbladder Cholangiocarcinoma: A primary tumor originating in the gallbladder, affecting its bile ducts, leading to cancerous growth. This form of cancer is relatively rare.
- Ampullary Cholangiocarcinoma: This Cholangiocarcinoma type originates in the ampulla of Vater, a small structure where the common bile duct and pancreatic duct join, leading to cancerous growth. It is also relatively rare.
Which are you?
Intrahepatic Extrahepatic – Perihilar Extrahepatic – Distal Gallbladder AmpullarUse the printable diagrams below to help or use the Patient Navigator Journals with your Doctor.
Must Do Checklist
What is your subtype? Can it be surgically removed? If not nan it be biopsied? If not can neoadjuvant treatment be used to shrink the tumour? Does your Medical Professional have current expertise and experience in your cholangiocarcinoma? Discuss obtaining a neutral second opinion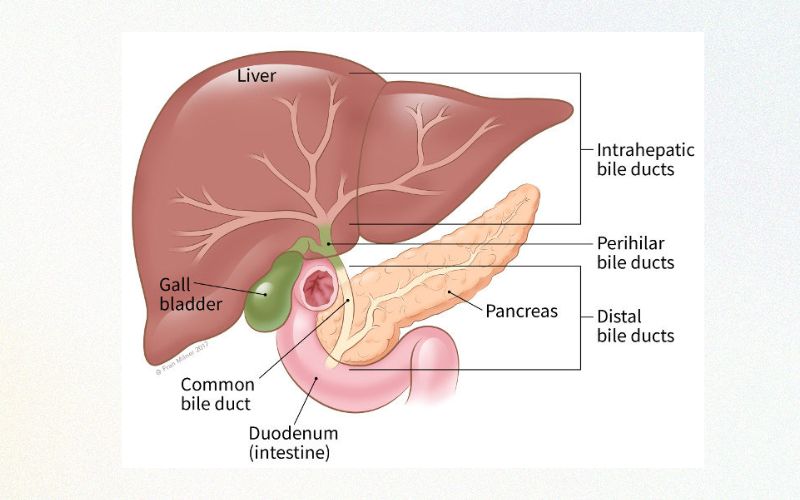

Understanding the stage of your cancer is a vital step in gaining a comprehensive understanding of your current condition. This process not only aids your medical team but also empowers you with valuable insights into navigating and measuring your journey effectively.
What you need to know
Determine whether the primary tumor remains stable and localised, if it has invaded the walls of the bile duct, or if it has spread to other locations (metastasis).
Staging the cancer provides critical information that directly influences your treatment options.
Why do you need to know
Comprehending the stage of your cancer empowers you to make informed decisions, communicate effectively with your doctor, and explore all available treatment options, including the potential for a complete and potentially curative surgical removal. It also instills a sense of control and confidence, enabling you to actively understand and participate in your treatment decisions.
Important note
Second and/or third opinions are vital at this point, so do not be afraid to ask for them. Second opinions should be unrelated to each other.Staging Attributes
HC (Immuno-histo-chemistry) is a rapid chemical staining test on tissue samples. This test is typically completed locally within 5 days, using tissue obtained from your surgery or a biopsy. Its purpose is to identify proteins found (expressed) on the surface of our cells, known as biomarkers. This provides evidence of the cell’s activity and can reveal known DNA mutations (mistakes) that are associated with certain types of cancerous tumours
What you need to know
Biomarkers are like clues about your cancer’s specific type, stage, and behaviour. They can also reveal genetic mutations that might be driving the cancer’s growth.
Why do you need to know
Knowing which biomarkers are present in your cancer can guide your medical team toward the most effective treatments, including cutting-edge immunotherapies. For example, if your IHC results show biomarkers like PD-L1, MSI-high, CTLA-4, HER2, or dMMR, you might be eligible for certain clinical trials targeting these exact features.
Important notes about these biomarkers
- T-cells act like our body’s security team.
- They have checkpoints on their surface, like CTLA-4 to prevent excessive activation of T-cells, also the y have PD-1
- PD-1 scans for PD-L1 on cell surfaces
- Healthy cells express PD-L1 to approaching T-Cells. When PD-L1 binds with PD-1 it deactivates the T-Cell attack
- This binding is known as “The Checkpoint Pathway”
- Cancer Cells can sometimes evade activated T-cells by expressing PD-L1 and deceiving the T-cell
- Immunotherapy drugs have been developed to block this pathway and binding to allow the T-cell to see and attack
*As a newly diagnosed patient, you must be aware of your biopsy’s biomarkers result. Is it a match for (ICI) “Immune Checkpoint Inhibitor” treatment? This is something you should know before committing to a treatment plan. If an IHC test is not helpful ask your oncologist to order a Genomic (Molecular) Profiling as your next option.
IHC Immuno-Histo-Chemical
- “Immuno-“ refers to the immune system and the use of components of the immune system, which includes antibodies that are used to recognize and bind to specific antigens (proteins) in the tissue.
- “Histo-“ comes from the Greek word “histos” meaning tissue. So, in this context, it refers to the study of biological tissues.
- “Chemistry” relates to the chemical reactions that occur when the antibodies bind to the antigens and the subsequent reactions that produce a visible signal, often a color change, which can be seen under a microscope.
So, Immunohistochemistry is a process that uses antibodies to detect specific antigens in tissues, and this detection is visualized through a chemical reaction that produces a color change. It’s like a highly specific and targeted coloring book where the antibodies are the markers that only color certain patterns (antigens) in the tissue. This allows doctors and scientists to see the presence and location of these antigens, which can be crucial for diagnosing diseases, including cancer.
IHC Attributes
Your Priority Checklist
What is your PD-L1 Score
What is your MSi Status
What is your MMR status – is it deficient? (dMMR)
Is CTLA-4 present
Is HER2 present
Genomic Profiling: A Roadmap for Personalised Treatments
Genomic profiling is a game-changer in cancer. If your IHC test doesn’t reveal suitable biomarkers for clinical trials, request Next Generation Sequencing (NGS), also known as Genomic or Molecular Profiling.
What you need to know
Biomarkers Matter- Genomic profiling identifies the genetic mistakes and mutations driving the growth of a tumor, and potential clinical trial treatments.
- Without a molecular profile, your oncologist can only use chemotherapy and radiation treatments, unaware of the underlying drivers of your cancer.
- Be prepared to wait 4-6 weeks for results.
- Blood biopsy can be used if tissue is not available.
Tumour Samples Types:
- Tissue from Surgery
- Tissue from a biopsy procedure,
- Blood Biopsy Option: Just know it’s not as spot-on as a tissue test.
This test also known as liquid biopsy, tests bits of material — like molecules or whole cells — that your tumor sheds into the blood, urine, or other body fluids. For some cancers, liquid biopsies can be used today to test for some of the same molecular features of cancer as tissue biopsies.
Why do you need to know
- Cholangiocarcinoma frequently presents actionable mutations, making genomic profiling vital. These mutations can be specifically targeted with immunotherapies.
- Identifying these mutations through profiling empowers your oncologist to create a personalised treatment plan aimed at eradicating the cancer.
Important notes
- Targeted immunotherapy, which identifies and attacks specific mutations driving cancer growth, is the future of cancer treatment.
- An oncologist with expertise in genomic profiling results and their relevance to ongoing clinical trials and treatment options is crucial.
- Biomarkers like PD-L1 expression, MSi, and TMB status can predict your response to immunotherapy and checkpoint inhibitor therapy, offering potential life-saving opportunities.
- Other relevant Biomarkers: CTLA-4 and HER2
Molecular/Genomic Profiling Attributes
- High rate of Actionable Mutations: Specific mutations can be targeted with available therapies.
- More effective treatment: Personalised treatments target the precise genomic alterations driving your cancer.
- Improved prognosis: Precision medicine improves overall prognosis and survival rates.
- Better response to treatment: Identifying specific genomic alterations helps identify potential treatment resistance.
- Clinical trial participation: Profiling can match you with ongoing clinical trials for potential life-saving treatments.
Further Explanation
In genetic studies, researchers examine an individual’s entire set of genes to identify inherited mutations or risk factors. In genomic studies, the focus is on the genes within cancer cells to pinpoint mutations driving cancer growth and determine the best treatment based on the tumour’s molecular profile.
In contrast, in genomic studies, scientists are focusing specifically on the genes in the cancer cells to identify mutations or alterations that are driving the cancer’s growth and to determine the best course of treatment based on the tumour’s molecular profile.
For more details click here
Your Priority Checklist
Order a Genomic Profile Highlight PD-L1 / MSi Status Highlight MMR status Highlight TMB Status Keep a copy of results on fileAfter diagnosing and staging cholangiocarcinoma, your doctor will discuss treatment options with you.
What you need to know
- Surgery is considered the sole potentially curative option.
- First-line treatment for cholangiocarcinoma is surgery. If surgery is not feasible, neoadjuvant chemotherapy followed by surgery and adjuvant chemotherapy with Gemcitabine/Cisplatin is the next option recommended.
- For inoperable cases, Gemcitabine/Cisplatin and radiation therapy are first-line treatments. Note; at the time of writing ‘Gemcitabine/Cisplatin/Durvalumab’ is first-line in the USA.
- Second or third-line treatments may include different combinations, even immunotherapy clinical trials.
Why do you need to know
- Understanding available treatment options is critical for making informed decisions that could really help improve your outcomes.
- Each treatment approach carries unique benefits and risks, with your specific situation guiding the best choice.
- Understanding these choices means you can have better discussions about these options with your doctor. Understanding empowers your real knowledge, and helps focus your research and decision-making.
Important notes
- Identifying relevant biomarkers like PD-L1, MSi-High, and TMB-High before treatment, especially for immunotherapy, is crucial.
- Early eligibility determination for clinical trials is necessary, as prior treatments may disqualify participation. Ensure your planned treatment won’t disqualify you from future trials.
Understand your treatment options
- Before starting any treatment plan – do you have biomarkers PD-L1, MSI-High, and TMB-High.
- Surgery is the only curative option for cholangiocarcinoma.
- Chemotherapy is a treatment designed to destroy all rapidly dividing cells, healthy or cancerous.
- Gemcitabine works by interfering with the growth and spread of cancer cells in the body.
- Cisplatin works by damaging the DNA in cancer cells, which prevents them from dividing and growing.
- Radiation Therapy uses high-energy radiation, such as X-rays or protons, to kill cancer cells.
- Targeted Therapies are treatments that target certain tumour cell parts that are fuelling cancer growth.
- Immunotherapy is a biological treatment that helps your own immune system fight cancer.
Explanations
- Neoadjuvant therapy is a treatment given before surgery to shrink the tumour and/or reducing the risk of cancer spread.
- Adjuvant therapy is administered after primary cancer treatment to reduce the risk of cancer recurrence
- Ineligibility for Surgery: Can a biopsy be obtained? Seek Second Opinions to be certain.
Your Priority Checklist
Doctor has Cholangiocarcinoma Expertise & Experience Surgery Eligibility Biopsy Eligibility Neoadjuvant then Surgery PD-L1, MSi-High, TMB-High mmunotherapy EligibilityUnderstanding the role of surgery in Cholangiocarcinoma treatment is crucial. Surgery is currently the only known curative option, but it may not be feasible in all cases, particularly if the cancer has metastasised.
Types of Surgery
Surgery options for bile duct cancer vary depending on tumour location, with different options for intrahepatic, perihilar, distal, and liver transplant cases. If surgery is not an option obtain a biopsy for molecular testing.
Surgical Options
- Intrahepatic: Liver Resection Surgery is an option if the tumour is located in the bile duct within the liver. Surgeons may remove up to 75% of a patient’s liver. Full liver transplants may also be an option in some cases.
- Extrahepatic – Perihilar: This location may require a combination of liver resection and Whipple surgery.
- Extrahepatic – Distal: Whipple surgery is an option if the tumour is located in the bile duct outside the liver, specifically in the common bile duct.
- Liver transplant: Surgery may be an option for some patients.
It’s important to note that surgical options may vary depending on the surgeon’s approach, experience, and risk analysis. A second or third independent opinion is common.
Important notes
It’s important to note that surgical options may vary depending on the surgeon’s approach, experience, and risk analysis. A second or third independent opinion is common.
Choosing your Surgeon
Choosing an experienced surgeon for Cholangiocarcinoma surgery is critical for optimal outcomes. Consider communication skills and seek a second independent opinion to ensure the best care.
Summarising surgery as a treatment
- Surgery is the only known curative option for cholangiocarcinoma, but eligibility depends on the tumour’s location, size, and stage
- Different types of surgeries are available depending on where the tumour is located, including intrahepatic, perihilar, distal, and liver transplant surgeries
- Neoadjuvant chemotherapy and/or targeted radiation may be used to reduce tumour size before surgery
- The choice of surgery depends on the surgeon’s approach, experience, and risk analysis
- Choosing the right surgeon with specific expertise and experience is critical for optimal outcomes, and it is recommended to seek a second independent opinion
- After surgery ensure that an IHC test is immediately conducted, highlighting PD-L1 score, MSi and MMR status and that there is also enough tissue sample remains for NGS profiling if/when required
Explanations
- Neoadjuvant therapy is a treatment given before surgery to shrink the tumour and/or reduce the risk of cancer spread
- Adjuvant therapy is administered after surgery to reduce the risk of cancer recurrence
Your Priority Checklist
Surgeon has CCA Expertise Curative Surgery Eligibility Neoadjuvant then Surgery Liver Resection Surgery Liver Transplant Surgery Whipple Multi-Organ SurgeryAre you a candidate or could you become a candidate for a Clinical Trial? Clinical trials are an essential component in a Cholangiocarcinoma patient’s treatment toolkit. They offer access to the latest cutting-edge treatments and opportunities.
What you need to know
Clinical trials are research studies aimed at evaluating a medical intervention. They are used to learn if a new treatment is more effective and/or has less harmful side effects than the standard treatment.
What you need to know
Clinical trials offer more options and opportunities when the current first-line treatment is not working. Clinical trials also offer you the opportunity to become involved in treatments that may well become tomorrow’s standard of care.
Important notes
It is important to prioritise consulting with an Oncologist who has the expertise and experienced with Cholangiocarcinoma and clinical trial options. Do not assume that your oncologist has the necessary experience, instead, ask them directly.
- Learn more about Clinical Trials
- Find a Clinical Trial
Trial Terminologies
- ORR (Objective Response Rate): The percentage of patients given a new treatment whose tumor shrinks or disappears by a certain amount within a defined period of time.
- PFS (Progression-Free Survival): How long a person keeps living without their cancer getting worse after starting a new treatment.
- OS (Overall Survival): How long a person keeps living after starting a new treatment.
Clinical Trial Phases
- Phase 1: First in Human trial – Focuses on safety issues like side effects, dosages, and how the drug works in the body.
- Phase 2: Focuses on both safety and the drug’s effectiveness. Typically lasts several months to a few years.
- Phase 3: Focuses closely on how well the drug works in a larger, specific population group of people and any side effects. Usually takes several years to complete.
Clinical Trial Attributes
- Innovative Treatment: Trials provide you the opportunity to become part of new options not yet available in standard care.
- Hope and Opportunity: Clinical trials provide structure and purpose to your hope, through access to new treatments and the potential for better outcomes.
- Clear Objectives: Clinical trials have well-defined and clear objectives that define the purpose and scope of the study.
- Monitoring and Surveillance: Clinical trials typically have more frequent and rigorous monitoring and surveillance protocols than standard of care treatments to ensure patient safety and to collect accurate data on the effectiveness of the treatment. Many patients see this as an advantage because it provides them with more personalised care and attention.
- Costs: Most Clinical Trials cover all your related costs.
Your Priority Checklist
Trial Eligibility Doctor has CCA experience Doctor has Clinical Trial experience Ask about Future Eligibilities Phase of trial – 1 , 2, or 3Second opinions can introduce new and potentially life-saving options, especially if the “Gold Standard” is not being followed.
What you need to know
A second opinion is another medical opinion from an independent doctor other than your current doctor and who has current Cholangiocarcinoma expertise.
What you need to know
Doctors can make mistakes or have varying opinions on the best course of treatment. Some can be too conservative, not up to speed and even fatigued. Getting a second opinion from another unrelated doctor with current expertise can provide peace of mind and potentially lead to a different treatment plan or diagnosis.
Important notes
Many doctors support their patients seeking second opinions. Additionally, consider remote second opinions to access a broader range of expertise, especially if travel is challenging.
Observations
The first diagnosis isn’t always correct or complete. According to a study by the Mayo Clinic, 88% of original diagnoses were changed or refined by a second opinion.
A second opinion can provide alternative options, which can benefit the patient physically, emotionally, and financially. Even just a confirmation of a diagnosis can provide peace of mind.
Second Opinion Attributes
- Expertise: The second opinion should come from a doctor who has current expertise in Cholangiocarcinoma and is experienced in providing second opinions. It’s important to seek a second opinion from a doctor who is knowledgeable in the latest treatments and research.
- Remote Opinion: The opportunity for a remote opinion increases the choice of more experienced oncologists with current expertise.
- Independent Opinion: The second opinion should be an independent opinion from a doctor who has no financial or personal ties to your current doctor or medical institution. This ensures that the opinion is unbiased and objective.
- Thorough Evaluation: The second opinion should be a thorough evaluation of your medical history, test results, and diagnosis. The doctor should take the time to review all relevant information and provide a detailed explanation of their opinion.
- Clarity: The second opinion should be clear and easy to understand. The doctor should explain their opinion in plain language and answer any questions you may have.
- Respectful: The second opinion should be given with respect and consideration for your feelings and concerns. The doctor should listen to your questions and provide compassionate care throughout the evaluation process.
Your Priority Checklist
Expertise & Experience Consider Remote Opinion Independent Opinion Thorough Evaluation Clarity + RespectfulMore Toolkit Resources
Know what questions to ask medical professionals
Simplifying and demystifying to increase your understanding

